
Americans Less Concerned About Drugs Than Ever: Poll
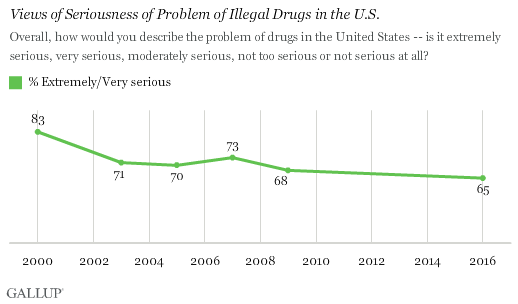
Sixty-five percent of Americans say that drug problems in the U.S. are “extremely†or “very serious,†according to a Gallup poll released Friday.
That’s the lowest level of concern the firm has found since it first asked the question 16 years ago, and it comes at a time when the county is experiencing what many experts have described as an “epidemic†of opioid overdose deaths.
Gallup attributes the drop in concern about drug problems nationally to younger adults, “who have never known a time when drugs were among the most prominent issues on the national landscape,†such as during the Reagan administration’s “Just Say No†campaign. “They have also come of age at a time when Americans, particularly those in their age cohort, support legalizing marijuana.â€
I would say it also has something to do with the work of drug policy reformers, who have actively and constantly countered both the stereotypes and the propaganda of drug warriors.
And there’s the reason that this lowering of concern, which I would also consider an increase in actual knowledge, is so good. It means that politicians and those who feed off the drug war trough now have a tougher time using “drug fear” to get what they want.
It used to be that all they had to do was say the word “drugs” and the Supreme Court, Congress, and the American people would bend over and relinquish rights, justice, and common sense. Perhaps that era has passed.

I’d say that there were other concerns for those politicians as well, such as the economy. It is becoming clearer to more people that the DrugWar is as I’ve always called it: a ‘rich man’s hobby’. And a country that has to decide on whether to buy groceries or pay their premium on ObamaCare isn’t rich, anymore.
Notice something, lately? How often do you hear the words ‘disposable income’ on the nightly news? They are hardly mentioned anymore in the LameStream Media, and for good reason, as it is virtually non-existent, save at the tippy-top of the economic pyramid.
And yet, from a national budget sense, that’s the only thing maintaining the DrugWar, the mistaken belief – or illusion – that we as a nation can still afford it. The reality has never been plainer that can’t. The fiscal chickens are coming home to roost, and they have razor sharp stainless steel beaks.
As predicted here so long ago, the economy is pulling the fiscal belt tighter to the point even the most demi-conscious, Pavlovian supporters of the DrugWar are dimly realizing that the money could go to better things…like the public support that so many are now on thanks to that same crappy economy.
As was said here long ago, ‘When it gets personal, it gets done’. The waste of taxpayer dollars on prohibition when formerly-employed Joe Blow needs those dollars for his food stamps is getting awfully personal.
And given the obvious economic boost legal cannabis has given Colorado, passing legalization referenda that use that rationale is more likely, especially in States that are feeling that economic belt-tightening. This issue, which those in power have been able to avoid for so long, is being pushed forward into the public mind in ways that are unavoidable. Because there’s only a couple of notches left on that belt before things get explosive.
And those iron chickens with razor sharp stainless steel beaks really do exist:
https://www.youtube.com/watch?v=wfsMZKwqw3w
Views of seriousness with regard to illegal drugs can be equated to hysteria. Mass hysteria is associated with a rise, a peak, and a decline. It’s like tyranny, as tyranny never lasts. Tyrants die or get replaced, and revolutionaries are always hard at work undermining a tyrant’s toxic mix of social and legal policies. With time and patience, the revolutionaries succeed.
An important point to note about hysteria is that it’s episodic. Throughout history pathological hysterias have been correlated with social catastrophes, only to subside and break out again with the next catastrophe. Examples include that of well-poisoning hysterias that caused communities to scapegoat lepers and Jews and burn them at the stake. Well-poisoning hysterias occurred in 1321 following the Albigensian Crusade, and again in 1348 beginning with Europe’s bubonic plague epidemic. (see David Nirnberg — Communities of Violence: Persecution of Minorities in the Middle Ages, 1998.) We have modern examples of alleged well poisonings here, along with issues about the use of well and spring water for marijuana production.
Many drug wars have existed throughout history, including those conducted by Roman men against women, and later by Christians operating under the Inquisitions who used prohibitions of local, ethnic, botanical substances to repress and enslave indigenous people in Central and South America. Anslinger’s, Nixon’s, and Reagan’s drug wars are part of a long historical list of political devices consisting of dual purpose laws that tyrants find useful for repressing or eliminating certain groups of people. As drug hysterias come and go, we’re seeing it go—for now. A better approach in the future would be to recognize mass hysteria at its outset and abort it before it causes further damage.
https://www.c-span.org/video/?417277-4/washington-journal-john-hudak-marijuana-legalization-ballot-measures
8:30am Washington Journal Oct.31
On Fresh Air– NPR radio transcript not yet up.
https://www.brookings.edu/book/marijuana-a-short-history/
Transcript up now.
http://www.npr.org/2016/10/12/497586908/how-the-cannabis-catch-22-keeps-marijuana-classified-as-a-harmful-drug
To add concern to this Halloween season the American Chemical Society brings us Death by Gummy Bears, a public health warning featuring the chemistry education series: Reactions–This is Chemistry:
https://www.youtube.com/watch?v=RNOycTzN-fg&feature=youtu.be
The LD-50 toxicity level for sugar is neatly explained (yes, it has one), making the standardized toxicology concept of LD-50 understandable to the lay public for other substances; for example, heroin.
What’s interesting about death by sugar overdose is that Gummy Bears containing THC would likely prevent the average sugar junkie from OD’ing, as the individual would fall asleep before reaching the minimum sugar toxicity or LD-50, thus preventing further sugar intake, and death. The dosage feature would work for children as well, making THC infused Gummy Bears safer than a straight up fatal shot of sugar.
Adding THC to Gummy Bears is also more moral than adding aviation fuel to ethyl alcohol to denature it and make it undrinkable, a method that’s resulted in 10,000+ deaths over the years. This means Kevin Sabet will need to focus his anti-drug propaganda on the dangers of Big Sucrose if he’s going to increase concern among parents with further fear mongering about Gummy Bears. He might even consider prohibiting Halloween, as it’s said Halloween candy can damage a kid’s teeth and lead them to try harder stuff, such as dextrose.
Catholic priests will still be free to sexually abuse little boys if adults can legally purchase and consume cannabis. And despite residents having a toke in the privacy of their homes, the Church will still frighten its members into increasing their tithes, and the USCCB will still attempt to control and dominate all American women. No reefer decriminalization will impact the Catholic ministry, but it will drastically reduce the number of people being arrested and imprisoned for marijuana possession, free up law enforcement to pursue nasty pedophile priests, and relieve America’s over-burdened judicial system.
http://tinyurl.com/NastyCatholicPedophilesAgainst
That is one powerful piece. If the members of a congregation wish to donate to influence an election, as private citizens, they have that right. A ‘religion’ is granted certain rights such as not paying taxes, in exchange for which they must keep to themselves. By interfering in an election, they have breached that social contract. If any ‘religion’ uses its members’ money to influence an election, it should lose its status as a ‘religion’, including being taxed as a regular business.
In 2015, Haslam lost his battle with cancer.
One month later, Kapalos quit her high profile media job.
In both his life and death, Haslam became the catalyst for Kapalos’ documentary, “A Life of Its Own”, — a film that provides clarity and understanding around medicinal cannabis — and something she describes as coinciding with a point in her life that she felt was an inevitable exit from media.
“I wanted to tell Dan’s story — the whole story — and the bigger issues that existed within it,” Kapalos said.
http://tinyurl.com/KapalosDocu
Pete, you have just regurgitated two articles in a row containing blatant propaganda about so-called “opioid overdose”. To follow the links in these articles is to bear witness to the methodology of propaganda making. As I said recently, this behaviour confirms you are a propagandist (along with Tom Angel). You are a propagandist because you know it is not true. The longer I read DrugWarrant, the more it confirms to me that you and the majority of your readers are exactly like the “prohibs” you claim to despise. The “prohibs” have their drug taking (alcohol, tobacco and caffeine) protected by law and engage in oppression of others who are engaging in exactly the same behaviour, except with different substances. The cannabis lobby fights for the “legalisation” of THEIR drug (cannabis) using the same oppressive methods used by the “prohibs” (propaganda about opioids). This amounts to nothing less than oppression (some would say violence) of other drug takers by the cannabis legalisation lobby: exactly the same behaviour that the cannabis lobby spends its life complaining about being the victim of. Disgusting behaviour and depressingly unceasing.
Matt, don’t forget to blame the commies for OD propaganda as well, FYI, “Severity of opiate intoxication to gender and age†by S. Shigeev, Department of Forensic Medicine Faculty of Medicine People’s Friendship University of Russia, Moscow:
Exactly right. To assert that the LD50 for morphine is 0.78 micrograms per millilitre is so absurd as to be beyond laughable. Terminally ill patients have blood morphine levels in the range of 0.5 to 3.
Matt, that LD50 estimate of .78 micrograms per milliliter is for an LD50, like it says. Not an “LD100.”
An LD50 amount is the quantity required to constitute a lethal dose for 50% of a given species population. An LD50 amount is approximate, not exactly precise. But it’s in the near vicinity. A closer approximation than Russian roulette.
Of course people who use opiates regularly, as with some terminal cancer patients, are usually able to sustain higher body loads of opiates. Regular users typically develop a physical tolerance, that’s well-known. In fact, the fact of opiate tolerance is as indisputable as the phenomenon of lethal overdose from opioids, opiates, and opium. But even at that, the latitude provided by tolerance is not all that great.
I support decriminalization of all personal drugs possession. I support heroin maintenance clinics (for addicts only.) But don’t condemn me for declining to support a commercial OTC market in a product as inherently risky and unsafe as the opioids.
The current success of cannabis legalization is the result of decades of sustained effort. If you want legalized opiates, organize and get your own movement. Don’t go off on some passive-aggressive rant, whining about the fact that others aren’t doing it for you.
But there’s a distinction in drug sensitivity noted in the Russian paper based on age. If other stats say people burn out on heroin addiction in their 30’s, and those who don’t dry out die out, then we’re looking at more subcategories that fall within particular age groups.
The variations in LD50 and LD100 based on age are presumably based on differences or changes in the human metabolism. These differences appear to be a real problem for heroin users. The elephant in the room appears to be that nearly everyone’s metabolism differs in some ways (mine certainly does), and it varies with age. Another problem, or variable, rests on the likely chance heroin users are not educated in advance in the science of toxicology.
Other variables emerge in understanding usage, such as the fact that teenagers are neurologically wired for taking risks — an evolutionary adaptive response, but one with a nominal death toll that ultimately benefits the group as a whole with new knowledge of what is impossible.
There are certainly strains of cannabis reform discourse that seek to demonize the “real drug users” in order to draw a distinction between cannabis and other psychoactive substances, and to suggest that law enforcement should “go after” some other group instead.
Most often, in my area, they point to methamphetamine, but heroin appears frequently, too.
So I agree there’s a basis for Matt’s perspective, but I disagree that Pete and his Couch are doing this in any significant way. If most current efforts are focused on cannabis, it’s because of its popularity and because of the clear injustice of its prohibition.
I do think we who support reform are likely to find ourselves divided, after federal cannabis prohibition falls, about where else our efforts should be directed.
I support decriminalization of opiates, but I think the next big frontier of reform should be psychedelics.
DC Reade: This is what you have said:”…is as indisputable as the phenomenon of lethal overdose from opioids, opiates, and opium.” Well its not true. You don’t understand the situation or you have a motive for telling a falsehood. The statement you have made is totally unsupported by evidence. There is only evidence to prove that what you have said is incorrect. If I ask for evidence to back up the statement you have made, nothing will be provided, because there is no evidence. It (fatalities with an opioid component) is NOT ‘overdose’. Tolerance plays no part in it. If a fatality is substance related, it is taking MULTIPLE drugs and becoming so sedated that airway obstruction results. Even a substantial “overdose” of (only) opiates does not result in this phenomenon (clinically proven).
It has nothing to do with passive-aggressive. The cannabis legalisation movement is furthering their own cause on the back of a lie. That is not good behaviour. They are engaging in the same behaviour that they are constantly complaining about being the victims of.
DrugwarRant is not “the cannabis legalisation movement”(how ever you define that). Should such a monolith exist however (and Kevin Sabet would say it does) would you please give us some citations and examples of how this “movement is furthering their own cause on the back of a lie.”
JV, you cannot be serious. DrugWarrant (it’s convener and majority of contributors) is/are obviously firmly slanted towards cannabis. To say otherwise is absurd. I think it is fair to say that DrugWarrant is part of the cannabis “legalisation” movement. Maybe lobby is the wrong word. Ever since I alerted Pete (and the readers) to the falsehood of fatal “heroin overdose” I have been treated with disdain, disinterest and internet bullying by one contributor in particular. The great majority of the readership is obviously not interested in the welfare of opioid users or the facts of the matter. An example? This exact article. This is what Tom Angel wrote (and Pete posted):
“That’s the lowest level of concern the firm has found since it first asked the question 16 years ago, and it comes at a time when the county is experiencing what many experts have described as an “epidemic†of opioid overdose deaths.â€
If you follow the link “many expertsâ€, you find an article commenting on the “…opioid painkiller and heroin epidemic…†A paragraph from it says:
“In 2014, nearly 19,000 Americans died from overdoses linked to opioid painkillers — sometimes opioids alone, other times involving drugs like alcohol and benzodiazepines (typically prescribed to relieve anxiety).â€
Surprise, surprise, the same bullshit describing multi-drug deaths as “overdoses linked to opioid painkillersâ€. And any brief investigation of the so-called “opioids alone†deaths (if they exist) will find low therapeutic morphine or opioid levels. So that JV, is the cannabis legalisation movement using a lie to further their cause.
Matt, this is just flim-flam from a closed mind. You haven’t provided any evidence at all for you obsessive one-track argument. By the way, you never answered my repeated questions from a year or two ago about how Dr Harold Shipman was able to murder a large number of his patients with a massive overdose of pharmaceutical diamorphine. According to your theory none of his patients should have died. I call b.s.
We can all agree that the reasons for prohibition of cannabis were lies and half truths. Unfortunately, the lies told about other drugs are still accepted as truth, even though we know about the cannabis lies. Why is it that so many in the legalization movement fall for this? I posit that exposure to cannabis is so common that ‘everyone knows’ about the lies, whereas many people, including myself, have no experience with heroin, meth, crack, ketamine etc. and therefore have not yet come to the conclusion that the supporting ‘reasons’ are in fact also lies. Is this not exactly the opposite of what we have preached for years; that children will come to know the cannabis lies for what they are, and assume that what they have been told about other drugs are lies also? Let us all assume that everything we have been told by authority figures , everything that we are being told by them, and everything that we ever will be told by them about all entheogenic drugs are lies. Then we may be open to the truth.
primus, some of us have made a habit of consulting the medical literature on various substances from the outset.
Unlike the case with the unfounded assumptions of legislators, police, and the mass media, the medical literature is usually accurate on most points- especially in recent years. When there’s controversy, it’s a good idea to read all of the viewpoints. But quite often, there is no dispute.
It’s as foolish to believe that all of the warnings about the risks and harms of drugs are lies as it is to swallow all of the claims unchallenged. Also considerably more reckless, if that viewpoint is taken as a guide for self-experimentation.
Of course, one should heed warnings regarding hazardous activities, however it does nobody any good to accept that the authorities’ pronouncements on other drugs are any more accurate than their pronouncements on pot. That acceptance of prohibition propaganda by our members when it relates to unfamiliar drugs, is what I was discussing. I, like the majority of us, have not read very much of the medical literature so cannot comment. What I have read a lot of is journalistic hyperbole and ominous pronouncements of impending doom from opportunistic politicians. In all cases, the drug was unimportant; all ‘drugs’ are lumped together for the purpose of social engineering. These warnings of doom by the press and politicians are of no value in this discussion, but can’t help but taint the thinking of all of us. We must be aware of these culturally cultivated biases and work to rid ourselves of them.
DC, you could do worse than listen to the wise words of Primus. Your words lead me to the crux of the issue. If authorities were really interested in “saving lives” they would communicate the reality: it is not opioid “overdose” that presents the problem, it is mixing drugs and airway obstruction. But they don’t, because they are out to perpetuate the myth of fatal opioid “overdose”. They are intentionally not communicating the truth. Because of their own self interest in the “drug war”, they cannot and will not tell the truth. And if they tell the truth, people will realize they have spent a 100 years lying. Do you not realise the authorities lie about drugs other than alcohol, tobacco and caffeine? The two biggest lies: fatal “heroin overdose” and cannabis causing schizophrenia. The foundation for a mass and long lasting human rights abuse.
You’re table-pounding, Matt. I challenge you to supply some well-grounded link or textual support for your contention that it’s “clinically proven” that opiates and opioids present no risk of overdose unless they’re mixed with other drugs.
It’s your claim. Don’t demand that I do your legwork to support it.
No DC you misunderstood, I demanded that you provide evidence of your claim. It is not up to me to provide evidence to back up a claim made by you. Anyway you won’t be able to do it because the evidence doesn’t exist. There is no evidence to support fatal “heroin overdose†when no other drugs are present. And no, the only time I pound the table is when I read a piece on DrugWarrant perpetuating the myth. I’m not making a claim, I am merely referring to a situation for which there is ample evidence. Now, the evidence: please look up- “Pharmacokinetics and pharmacodynamics of high doses of pharmaceutically prepared heroin, by intravenous or by inhalation route in opioid-dependent patients.†“Overdoses†of 150% given to subjects that were also on methadone treatment. They barely flinched. Neither the researchers or subjects new the dose. Maximum IV dose given: 450mg. So thats a 150mg “overdose†given to a subject on a 300mg maintenance dose. And don’t come back with the old chestnut of “they were tolerant†because opiate naive people are not the people typically involved in deaths in which heroin metabolites are found. Again, it is long-term tolerant users usually involved. They have either died of causes unrelated to substance use or have mixed drugs, become heavily sedated, suffered airway obstruction and suffocated. If you require anymore evidence don’t hesitate to contact me via this site.
The best experimental evidence comes from Drs. Lawrence Kolb and A. G. Du Mez of the United States Public Health Service; in 1931 they demonstrated that it takes seven or eight milligrams of heroin per kilogram of body weight, injected directly into a vein, to kill non-addicted monkeys. On this basis, it would take 500 milligrams administered in a single injection to kill a non-addicted human adult.
Source: Lawrence Kolb and A. G. Du Mez, U.S. Public Health Reports, 46 (1931): 698
Matt, you’re indulging in sophistry as if you’re trying to win a prize for it.
You don’t get to cherry-pick one study, interpret the findings to suit yourself, and slam the discussion shut. The fact that addicts in a methadone program were able to survive a relatively large dose of heroin is practically meaningless- methadone is favored in drug maintenance programs partly due to its heroin-blocking effect! (I seriously doubt that the phrase “they barely flinched” was found in the language of the report.)
And you’re standing the evidence on its head when you start playing games like this: “don’t come back with the old chestnut of “they were tolerant†because opiate naive people are not the people typically involved in deaths in which heroin metabolites are found.”
“Opiate-naive people” are most certainly found within the population of lethal opioid overdose cases. Enough of them to falsify your insinuation. Which is false, in any case- no one is implying that tolerance confers total immunity from heroin overdose- only some additional protection, to an uncertain effect.
You don’t get to rely on a couple of studies and rule all of the other evidence out of bounds, Matt. Especially when the studies you use to support your claim aren’t saying what you imply they’re saying.
Back in the seventies when I was first scripted for methadone I was told that if I took heroin on top of it, it would be like “washing my feet with my socks on,” i.e. I wouldn’t get a high [Brendon at Paddington DDU]. That wasn’t quite true but there was certainly a dampening down of the opiate high associated with methadone use.
Jake, you can’t reliably posit a 1:1 correspondence between monkeys and humans. The weight difference alone implies metabolic dissimilarities.
There’s also something terribly idiosyncratic about the way that opiates and opioids produce lethal effects. They suppress the respiratory reflex. That isn’t an entirely dose-dependent effect. The fact that some people are able to survive a very high dose amount on a given occasion does not clear them of the hazard of overdose. They kill reliably enough to be considered lethal drugs.
Matt asked for scientific evidence to support the possibility that it’s possible for a human to overdose using just heroin. If you have anything better than what Lawrence Kolb and A. G. Du Mez presented back in 1931 then please get back to us with it.
I think we can safely assume that they killed far more than just one non-addicted monkey to reach the magic number of seven or eight milligrams of heroin per kilogram.
Is Matt sparked-out behind the couch again?
Your data is valid, Jake. My point is that as with most CNS drugs, opiate/opioid OD isn’t strictly correlated to dose or blood level. Anything more than a low dose begins introducing an element of chance of respiratory suppression that can go terminal.
It isn’t easy to study something like this, for some quite sensible ethical reasons, but anecdotal evidence of opiate ODs from smaller amounts than .5 grams is plentiful. A sample:
https://drugs-forum.com/forum/showpost.php?p=1514046&postcount=16 (100mg levo-methadone)
https://drugs-forum.com/forum/showpost.php?p=1660322&postcount=35 (Two MS Contin pills total only 30mg morphine, according to this data sheet: https://www.drugs.com/dosage/ms-contin.html )
Matt is correct that mixing opiates with any other CNS depressant potentiates the effect massively. Most ODs do involve a multiple drug combination, including most of the ones in the thread from which I extracted those posts: https://drugs-forum.com/forum/showthread.php?p=1660322#post1660322
DC Reade, this conversation has followed a predictable course that unfortunately has been the norm for this subject on this site previously. Your methods in the main are three-fold. Firstly you attempt to discredit irrefutable evidence that an “overdose” of opioids when people have only opioids in their system is not dangerous. I doubt whether you even bother to read such evidence. Secondly, you fail to provide evidence of so-called fatal “heroin overdose”. Your attempt to provide some sort of evidence in the form of two forum anecdotes is tragically laughable. Thirdly, you offer outright falsehoods such as your first paragraph. What utter rubbish. What is important is your motives. You are clearly intent on assisting the continuance of a human-rights abuse commonly referred to as the War on Drugs. Maybe you get paid to do it. I can only wonder.
Oh, I can find more anecdotes.
I’ve done enough research on opiate/opioid overdoses to know for certains that lethal consequences from ingestion occur even in the absence of other drugs or toxic contaminants. And while the conundrum that 1) lethal overdoses have been found to occur even with much lower quantities than those that are supposed to be necessary to produce death and that 2) it’s possible for people to ingest very high levels of opiates/opioids without suffering the consequence of terminal respiratory depression is a medical mystery,it isn’t “proof” of the harmlessness of opiate/opioid narcotics. It certainly isn’t reassurance that there’s no such thing as a lethal dose; it’s at least as reasonable to assume that opioids and opiates interact with the human body in ways that can’t be predicted with foolproof certainty- especially not with, shall we say, 100% accuracy over the course of 1000 or 10,000 different occasions of ingestion.
It’s also the case that post-mortem toxicology reports do not do a reliable job of gauging blood levels for some drugs, and hence are not reliably able to judge the quantity of ingested material:
“…While postmortem redistribution may elevate drug concentrations in blood, some drugs continue to be metabolized after death. Enzymes, especially esterases, that do not require oxygen or consume energy, remain active and hydrolyze susceptible drugs, including cocaine, heroin and a heroin metabolite, 6-monoacetylmorphine. The net effect of the competing processes, redistribution and metabolism, on drug concentrations in postmortem specimens is unpredictable…”
http://what-when-how.com/forensic-sciences/interpretation-of-results/
Absolute malicious, unsubstantiated rubbish. And I bet you can sleep at night. Again and for the last time, the one thing you lack is evidence.
“…According to toxicological information, the toxic range for heroin is >0.08 mg/L, and the fatal range is 0.08–1.6 mg/L. These figures refer to non-drug tolerant individuals but will be used as the basis for classifying data in this study. One hundred and thirteen people (80%) had a heroin level in the fatal range. Another eight male cases (6%) had heroin levels above 1.6 mg/L. The mean total blood morphine was 0.29 mg/L. Thirty-five percent of the cases had a bile morphine level of greater than 40 mg/L. As discussed below, this implies “chronic usage.†Most of this group (96%) also had heroin levels that were greater than 0.08 mg/L, within the fatal/toxic range, and 91% were male.
The toxicological screen showed that a high proportion (43%) had evidence of multiple drug use…”
i.e., 57% did not show evidence of multiple drug use.
Plenty more context, here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4519229/
I am saddened by this bickering. Can we not all agree that there is a tremendous amount of misinformation out there, propagated by the prohibitionists in the main, which is affecting the discussion? All of us, Matt and myself included, have believed misinformation and incorporated it into our thinking. We don’t really know definitively which nuggets are true and which are false. Even those of us who are well educated on the subject of drugs, their effects and legal status, are prone to this error. When someone challenges our long-held beliefs, it is natural to resist. It is the challenger’s responsibility to present information supporting the challenge, and try to persuade others of the validity of the challenge. It appears that Matt, Cj and others have failed to accomplish this persuasion. It is not my fault that you have done a poor job of presenting your arguments, it is yours. My job is to be a skeptic and seeker of truth. When you convince me of the truth of your position, I will happily change my mind and incorporate the new information into my thinking. Until then, try not to take this resistance personally. I am glad of your interest and information. Please try to understand why you meet resistance and work hard to overcome it. It’s worth the effort. Once you convince us, we will become ardent ambassadors spreading your words and ideas for you.
Matt, you still owe us all a reply to my above post.
Here it is again:
The best experimental evidence comes from Drs. Lawrence Kolb and A. G. Du Mez of the United States Public Health Service; in 1931 they demonstrated that it takes seven or eight milligrams of heroin per kilogram of body weight, injected directly into a vein, to kill non-addicted monkeys. On this basis, it would take 500 milligrams administered in a single injection to kill a non-addicted human adult.
Source: Lawrence Kolb and A. G. Du Mez, U.S. Public Health Reports, 46 (1931): 698
Matt, do you still insist that there’s no such thing as a lethal heroin dose?
… sound of crickets chirping ..
Matt, If you turn up here again, hurling personal abuse and claiming heroin has no fatal dose, I’ll kindly remind you that you never responded to this post, and not once but twice. What’s it to be, Matt?
Jake, “hurling personal abuse”? Now you know that’s not true. Anything that challenges the belief system of DWR contributors is usually classified as personal abuse. I never said “…there’s no such thing as a lethal heroin dose”. It is possible to fatally overdose on water for instance. Again, it has been conclusively proven that heroin is safe in substantial overdose (150%). I doubt anyone here even read the study I provided the name of. It may be possible to die from the effects of morphine, but there is no evidence to even suggest it happens as a result of recreational heroin use. Unfortunately, it is pretty much a pointless exercise to discuss the issue here as none of the regulars or the convener are interested despite saying they are against the “drug war” in general. Lets face it, it is just cannabis self-interest here. If they were interested there would be none of the denial and argumentative behaviour when the subject is brought up. So no, Jake, no crickets, just the truth, which most people apparently can’t handle.
Matt: I think you may be reading too much into this. I remarked in an earlier post that you have not made your case. That is a part of it. You are correct when you say that we are focused on cannabis prohibition. That is true. An old saying is that politics is the art of the possible. What is possible now, mainly as a result of a lot of work on our parts, is the legalization of cannabis. What is not possible at this time is the legalization of opioids. That fact is far more important than your frustration at not having your ideas readily accepted. Your frustration is more than matched by ours; Cannabis consumers far outnumber opioid users and the reasons for its prohibition are weaker than the reasons for opioid prohibition. The reputation of opioids is much worse mainly because it is linked with death. Cannabis is not, nor ever will be. It is actually impossible to die of a cannabis overdose. Your protestations that opioids are just as safe ring hollow when ‘everyone knows’ that opioids can be lethal. When something which is proven non-lethal is prohibited, it is much easier to persuade the public of the need of change. For opioids to be similarly viewed, cannabis must be legalized, and the public must see that the sky does not fall. Only then will they be willing to entertain the concept of total drug legalization, a concept shared by myself and many other DWR reader/writers. In the meantime, we all have a huge educational mountain to climb. It has taken my entire adult life (now 64) to overcome society’s misconceptions about cannabis. Be prepared for it to take that long or more for opioids to be similarly accepted. One can, of course hope that it won’t take as long, but it very well might. Be frustrated but work towards your goal. That is the only method that will work. That is what we Cannabis Crusaders have done for many years. Railing against and criticizing the limits of we who are working towards our goal will not assist you to reach yours. Keep Calm and Carry On.
“Anyway you won’t be able to do it because the evidence doesn’t exist. There is no evidence to support fatal “heroin overdose†when no other drugs are present. And no, the only time I pound the table is when I read a piece on DrugWarrant perpetuating the myth.”
Those were your words, Matt.
More than half-way down this thread:
http://www.drugwarrant.com/2016/10/people-are-less-concerned-about-drug-problems-and-that-can-be-a-good-thing/
â€You are clearly intent on assisting the continuance of a human-rights abuse commonly referred to as the War on Drugs. Maybe you get paid to do it. I can only wonder.
—Your reply, Matt, to DC Reader
â€You have known for a long time that there is no such thing as (fatal) “heroin overdose†or “heroin-related overdose†yet you continue to be either obstinately gullible or an outright propagandist yourself.â€
-Your response, Matt, to Pete’s post titled: Smart approaches to heroin problems talked about in mainstream media?
That’s not the usual way we talk to each other on this couch, Matt. Maybe you should look for a different forum? One where they’ll better appreciate your abusive mannerisms.